One-lung ventilation (OLV) is a specialized anesthetic technique commonly used during thoracic surgical procedures to allow the surgeon access to the operative lung while the other lung continues to provide ventilation and oxygenation. For anesthesia coders, understanding how and when OLV is used helps clarify why certain anesthesia CPT codes apply—particularly ASA 00541.
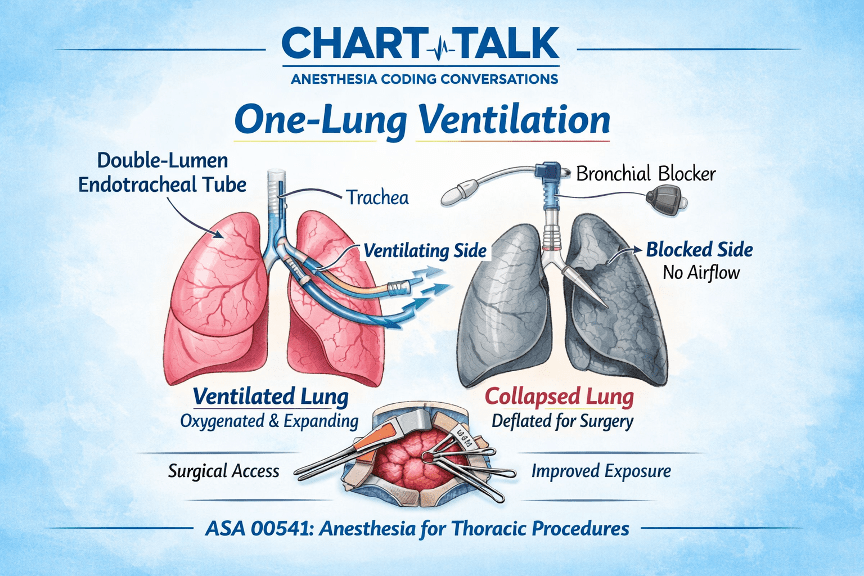
One-lung ventilation (OLV) is a ventilation technique where one lung is intentionally collapsed (the operative lung) while the other lung continues to be ventilated by the anesthesiologist. This technique improves surgical exposure and safety during thoracic procedures.
Collapsing the operative lung allows better visualization of the surgical field, more space for surgical instruments, reduced movement from lung expansion, and improved precision during thoracic surgery.
OLV is achieved using lung isolation techniques. The two most common methods are:
1. Double-Lumen Endotracheal Tube (DLT) – A specialized airway tube with two lumens allowing independent ventilation of each lung.
2. Bronchial Blocker – A device inserted through a standard endotracheal tube to block ventilation to one lung.
OLV is frequently required for thoracic procedures such as lobectomy, pneumonectomy, thoracoscopy (VATS), esophageal surgery, mediastinal procedures, lung biopsy, decortication, and bullectomy.
ASA 00541 describes anesthesia for thoracotomy procedures involving the lungs, pleura, diaphragm, and mediastinum. One-lung ventilation is included in the anesthesia service when performed and is not billed separately.
– OLV is included in the anesthesia service
– It is not separately billable
– Code selection is based on the surgical procedure
– Documentation should reflect the thoracic procedure requiring lung isolation
When reviewing anesthesia records, coders may see terms such as: double-lumen tube placed, lung isolation achieved, bronchial blocker used, one-lung ventilation initiated, or operative lung collapsed for surgical exposure.
While one-lung ventilation is not coded separately, recognizing it in the anesthesia record helps coders understand the complexity of thoracic anesthesia services and supports appropriate anesthesia CPT code selection.
DISCLAIMER: Chart Talk: Anesthesia Coding Conversations is intended for educational and informational purposes only. The information presented reflects the sole interpretation and professional opinion of the presenter. It does not represent the views or official guidance of my employer, the Centers for Medicare & Medicaid Services (CMS), the American Medical Association (AMA), or any other regulatory or governing body.
Every reasonable effort has been made to ensure the accuracy of the information provided at the time of publication. However, coding guidelines, regulations, and payer policies are subject to change. It is the responsibility of the reader or participant to verify current guidance and apply professional judgment when making coding and billing decisions.
— Dianne
Chart Talk: Anesthesia Coding Conversations

Leave a comment