Post-operative pain management continues to evolve, and ilioinguinal and iliohypogastric nerve blocks are commonly used regional techniques—particularly for lower abdominal procedures. While clinically effective, these blocks often raise coding and documentation questions, especially when they are performed together.
What Are Ilioinguinal and Iliohypogastric Nerve Blocks (CPT 64425)?
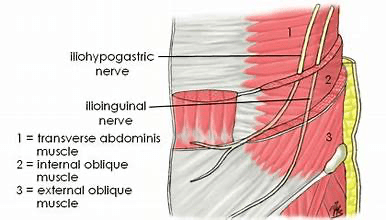
The ilioinguinal and iliohypogastric nerves originate from the L1 spinal nerve and provide sensory innervation to the lower abdominal wall, groin, and upper thigh region. Because of their close anatomical relationship, these nerves are frequently targeted together to manage post-operative pain.
Common procedures where these blocks may be used include:
• Inguinal hernia repairs
• Cesarean sections
• Appendectomies
• Gynecologic and lower abdominal surgeries
Single Injection vs. Two Separate Blocks
From a clinical standpoint, these nerves may be anesthetized with one injection at a single fascial plane or with two injections targeting each nerve individually. This distinction is critical for coding purposes.
Just because two nerves are involved does not automatically mean two separately billable blocks.
Coding Considerations
When ilioinguinal and iliohypogastric nerve blocks are performed, they are commonly reported as a single abdominal wall nerve block. When performed together via the same injection site, only one block is typically supported.
Separate reporting may only be considered when documentation clearly supports distinct injections, separate needle placements, and medical necessity for treating each nerve independently.
Documentation Elements to Look For
To support appropriate billing, the anesthesia record should include:
• Identification of the nerves blocked
• Laterality (if applicable)
• Technique used (ultrasound guidance or landmark-based)
• Number of injections and needle placements
• Purpose of the block (post-operative pain management)
Auditor’s Perspective
From an audit standpoint, the key is combining clinical reality with documentation support. If the record reflects one injection targeting both nerves with no distinction between separate techniques, reporting a single nerve block is generally appropriate.
This is another area where coding is not always black and white and where professional judgment plays an important role.
Final Thoughts
Ilioinguinal and iliohypogastric nerve blocks are effective tools in post-operative pain management, but they require careful review when it comes to coding and compliance. Understanding anatomy, technique, and documentation expectations helps ensure accurate reporting and audit defensibility.
Educational Use Disclaimer: This material is for educational purposes only and does not constitute billing or legal advice. CPT and coding guidance should always be applied in accordance with payer-specific policies and official guidelines.
DISCLAIMER: Chart Talk: Anesthesia Coding Conversations is intended for educational and informational purposes only. The information presented reflects the sole interpretation and professional opinion of the presenter. It does not represent the views or official guidance of my employer, the Centers for Medicare & Medicaid Services (CMS), the American Medical Association (AMA), or any other regulatory or governing body.
Every reasonable effort has been made to ensure the accuracy of the information provided at the time of publication. However, coding guidelines, regulations, and payer policies are subject to change. It is the responsibility of the reader or participant to verify current guidance and apply professional judgment when making coding and billing decisions.
— Dianne
Chart Talk: Anesthesia Coding Conversations

Leave a comment